

Salvaging the COVID-19 Vaccine Narrative
The Norwegian Study and others that seek to deflect attention from troubling trends
Many countries worldwide have experienced excess all-cause mortality (ACM) that coincides temporally with the COVID-19 mass vaccination campaigns. In a seeming attempt to salvage the “safe and effective” narrative, several studies have emerged to counter the conjecture that the COVID-19 vaccines may increase mortality risk. A recent preprint out of Norway (Dahl et al., 2024) presents one such study.
The authors compare the all-cause mortality rates between vaccinated and unvaccinated individuals aged 18 years or older living in Norway during January 1, 2021 through to December 31, 2023. The study used individual-level data where individuals were categorized as either unvaccinated (received no doses), partially vaccinated (received one or two doses) or fully vaccinated (received three or more doses) from the date of vaccination and onwards. Based on their analysis, the authors conclude that vaccinated individuals had a lower rate of all-cause death during 2021-2023 in Norway, even after accounting for sex, calendar time, county of residence and a high-risk health indicator. The authors cite several other supporting studies that have concluded there was no observed increase in all-cause mortality in vaccinated individuals.
While it may seem that these studies are evidence that the COVID-19 vaccines reduced mortality (or at the very least did not contribute to it), that is not the case. Contained within these papers is evidence (falsification tests) that betray such a conclusion. In the end, these studies serve to highlight the inherent limitations of observational studies and demonstrate their potential for misuse. This is particularly problematic for those seeking to show that the C19 vaccines are “safe and effective,” a claim that was not sufficiently established during the clinical trials.
On the flip side, the spectacular willingness of journals to publish studies with misleading conclusions in support of the highly politicized “safe and effective” claim provides additional fodder for those exposing the feeble science behind such assertions.
Troubling COVID-19 Trends Following Vaccination
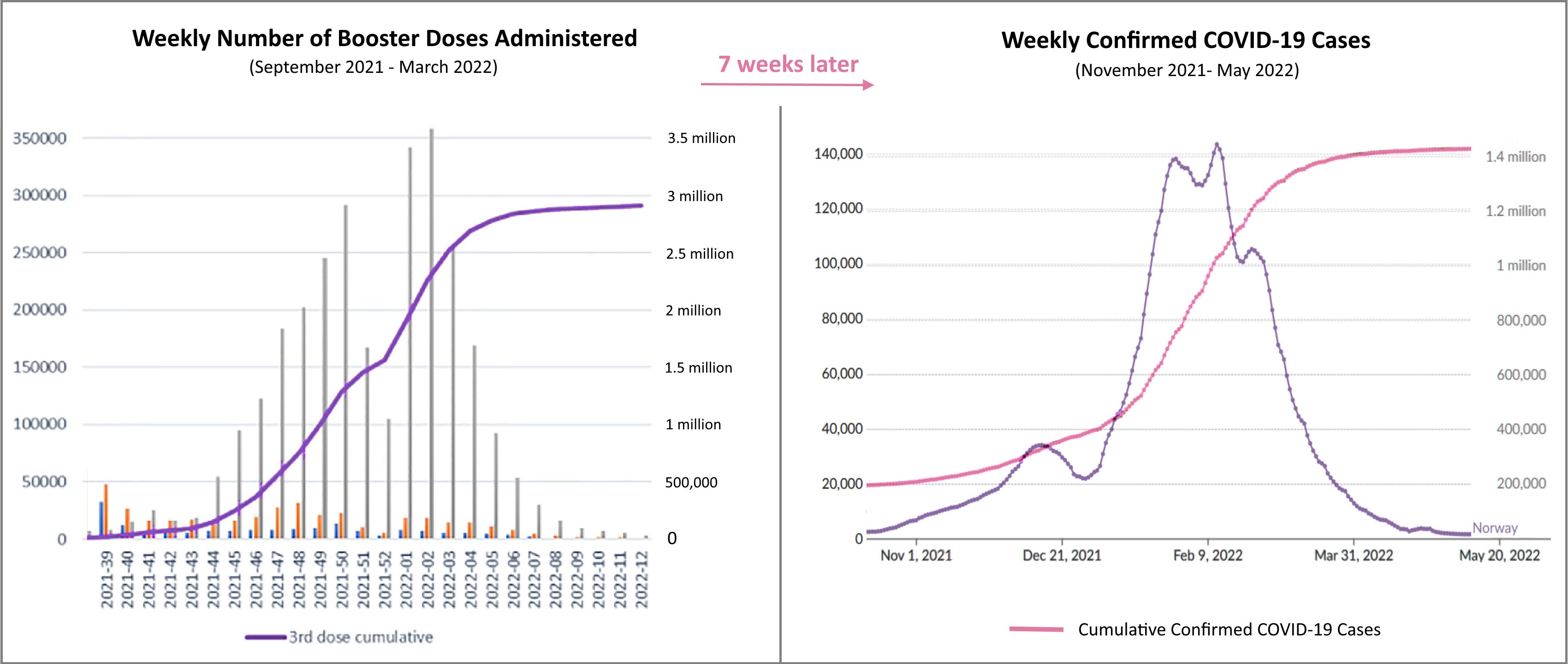
In Norway, administration of the first and second-doses of the COVID-19 vaccines ramped up in the spring of 2021, plateauing by the end of summer with just over three-quarters of the population having received at least one dose and with second doses nearing 70%. Up to that point, the country had experienced relatively few COVID-19 cases and no excess deaths (upper left and lower right panels in the figure below, respectively).
Booster doses began ramping up in October 2021. Seven weeks later, Norway began to see a surge in cases that reached shocking heights in January and February 2022 before subsiding towards the end of March. This was followed by an increase in COVID-19 deaths in December 2021 and throughout 2022 (lower left panel).

The plot below shows the rollout of the C19 booster doses administered in Norway (left panel) and the subsequent rise in the number of confirmed cases just 7 weeks later (right panel). By mid-November 2021 (20 months into the pandemic), Norway had reported 230,000 total cumulative cases since the beginning of the pandemic. Just 4.5 months later, with about 80% of the population having received at least one C19 dose and over half the population boosted, the total cumulative cases was over 1.4 million (over 25% of the total Norwegian population).
In the figure below, the plot of the cumulative number of C19 boosters administered in Norway is overlayed with the cumulative number of C19 cases that occurred 7 weeks later. Interestingly, the rise and timing in cases almost perfectly matches the uptake in C19 booster doses just weeks before. While the strong correlation doesn’t mean the booster rollout caused the subsequent rise in COVID-19 cases, this plot is still pretty damning. It would be difficult to argue that the vaccines had any protective effect on COVID-19 infection — the evidence suggests the contrary.

No increase in excess ACM until the C19 vaccine rollout
Mid-way through the core vaccination period in the summer of 2021, when half of the population had received at least one dose of a C19 vaccine, Norway began to see a steady rise in cumulative excess all-cause mortality. As shown in the plot below, excess mortality persisted even after COVID-19 deaths tapered off, indicating that something more was driving the increase in ACM.

A look at excess ACM by major cause of death reveals a pronounced increase in cardiovascular diseases during the vaccine rollout. While the causal link between cardiovascular injury and the genetic injections is well-documented, authorities have downplayed the potential magnitude of this risk and have stayed clear of insinuating that the vaccines may be a contributing factor for the observed increases in excess ACM.
The cumulative excess number of deaths in Norway by major cause of death for 2020-2022 is presented in the graph below (left). Apart from COVID-19, excess mortality was most pronounced for cardiovascular diseases in both 2021 and 2022. Monthly age-standardized mortality rates (ASMR) and the cumulative excess ASMR from cardiovascular diseases is presented below (right).

Problems with Estimating the Impact of C19 Vaccination
As demonstrated above, prior to the administration of C19 booster doses in the fall of 2021, Norway experienced relatively few COVID-19 cases and no excess all-cause deaths during the first year-and-a-half of the pandemic.
In 2021, the vast majority of deaths had nothing to do with C19 nor the vaccines. The predicted number of all-cause deaths based on pre-pandemic trends from 2010-2019 was 40,241 deaths versus the observed number of 41,713 deaths — an increase of about 3.7%.
In 2022, Norway experienced the largest reduction in life expectancy since World War II and excess mortality rose to an estimated 14.5% (Raknes et al., 2024).
Considering that overall COVID-19-related deaths represent a very small portion of total deaths (about 2% in 2021 and just over 6% in 2022) even if it is assumed that vaccination is highly effective at reducing COVID-19-related deaths, this will affect the risk of all-cause deaths only marginally. Without a proper baseline, the impact of vaccination will be overshadowed by a multitude of other factors — confounding will be a major problem.
In a randomized control setting, measuring the impact of vaccination would be much simpler. People would be randomly assigned to either a vaccine group or placebo group so that confounding factors would more or less even out, the only main difference between the two groups would be whether or not individuals received the vaccine. Then, under similar conditions (ie. the same exposure to COVID-19 and no vaccine-related policies that favored one group over the other) any increase or decrease in the ACM of the vaccine group relative to the placebo group over the study period could be attributed to the effects of the vaccine.
But real-world data is much, much messier.
Not only do the two groups differ in key attributes, but the characteristics of the groups themselves change over the course of the vaccine rollout, as do environmental and political stressors (pandemic policy), the type of vaccines distributed and their administration, the treatment of COVID-19 patients, the level of healthcare services available to the public... It’s a confounding mess!
First consider how the vaccines were rolled out. Before universal access was achieved for the entire population, priority was given based on age, medical risk status, occupation and place of residence (Skjesol and Tritter, 2022). Thus, as the vaccines were rolled out there have been dramatic shifts in the age, health and socio-economic composition of both the vaccinated and unvaccinated groups, especially throughout 2021.
Next consider the demographic and socio-economic attributes associated with those less likely to take the vaccine. COVID-19 vaccines were offered to all residents in Norway on a voluntary basis, free of charge. Nonetheless, lower household income was associated with lower C19 vaccine uptake (Hansen et al, 2023). Moreover, Foreign- and Norwegian-born persons with foreign-born parents (about 18.9% of the total population) had lower COVID-19 vaccine coverage than those who were Norwegian-born with Norwegian-born parents. This remained the case even after adjusting for income, education, sex, age, medical risk group and place of residence (Kraft et al, 2025). Furthermore, there was considerable variation in COVID-19 vaccine coverage between different immigrant groups:
As of October 2021, vaccination coverage for different country backgrounds varied from around 45 % for persons from Latvia, Bulgaria, Poland, Romania and Lithuania to 92 % for persons from Vietnam, Thailand and Sri Lanka. Those in the former group had from 15 to 18 times higher odds of not having been vaccinated as persons with a country background from Norway.
As of 20 October 2021, 94 % of Norwegian-born individuals with Norwegian-born parents had received at least one vaccine dose. Rates amongst Norwegian residents born in Sweden and Denmark were similar to Norwegian born.
These disparities are quite significant, especially since both lower income and immigration status have been linked to poor COVID-19 outcomes:
Lower socioeconomic groups were more often infected and had higher risk of severe disease – hospitalization, ventilator use and death.
Immigrants have been found to have higher reported rates of COVID-19 and related hospitalizations than non-immigrants (Arora et al., 2022);
Those who were foreign-born make up around 15% of the population, but accounted for around 40% of all hospital admissions from COVID-19, from March 2020 to February 2021, and this varied greatly by country of birth (Institute of Health Equity, 2023). This overrepresentation extends to deaths due to COVID-19 (Benavente, Ronda & Diaz, 2023).
Many studies have acknowledged that the population of vaccinated individuals differs in meaningful ways from those who chose not to take the new C19 pharmaceuticals. A myriad of factors impacts one’s mortality risk: age, living conditions, finances, employment, working conditions, housing standards, social participation, general health, major life stressors and so on. Both the baseline and the progression of these factors over the course of the pandemic differ for vaccinated and unvaccinated groups.
The situation is further compounded by major changes in public policy that caused huge disruptions in the economy, health services and social interactions — the burdens of which were more pronounced amongst migrants and low income households. Social pressures and consequence of remaining unvaccinated may also play a role, though perhaps not to the extent it did in countries like Canada were the unvaccinated were severely punished.
The epidemiological progression of SARS-CoV-2 and its impact on the transmissibility and severity of disease also must be accounted for in the modeling, as exposure rates and health risk changed over time. And of course seasonality plays a role in mortality risk.
With such a dynamic, complex system at play, a key modelling question is: How did researchers account for this massive confounding and what, if any, meaningful inferences can be made?
The Norwegian Study — A Confounding Mess
Based on their simplistic analysis, Dahl et al., 2024 conclude that vaccinated individuals had a lower rate of all-cause death during 2021-2023 in Norway compared to those who did not take the C19 vaccine, even after accounting for age, sex, calendar time, county of residence and a simple indicator denoting high health risk.
Did they establish baseline mortality trends for the two groups? No.
Do they control for massive confounding? No.
Do they offer any explanation for the concomitant increase in excess ACM with the vaccination rollout? No.
While the authors do not claim the vaccines themselves are responsible for the lower all-cause mortality amongst the vaccinated group, it is strongly implied in their publication and they neglect to discuss the myriad of factors apart from vaccination that are likely contributing to the difference.
So, what does their analysis actually show? — It shows the vaccinated and unvaccinated groups differ in key attributes (above age, gender, and a broad-based health indicator) that are related to, or impact, mortality risk. Something we already knew.
It should be obvious based on the discussion in the previous section that the researchers’ thoughtless handling of confounding issues by adding a few problematic covariates into their statistical software package was grossly insufficient. That said, Supplemental Table 2 of their report, which provides unadjusted and adjusted incidence rate ratios of death (all causes) by vaccination status and year, does provide a falsification check of sorts.
The Norwegian Study: No baseline. No controls. It’s a Confounding mess! This study and others like it just serve to obfuscate, distract & divert attention from problematic trends following the C19 vaccine rollout.
A Falsification Test of Sorts
As discussed earlier, the majority of the Norwegian population wasn’t vaccinated until the second half of 2021. Moreover, COVID-19 cases and subsequent deaths remained very low throughout 2021 until rising in Nov-Dec with the rollout of booster doses; the large spike in both cases and deaths occurred in the early months of 2022. That is, COVID-19 posed a relatively small risk to the Norwegian community during the 2021 calendar year, its contribution to overall all-cause mortality and the protective effect of the vaccines, if any, would’ve been quite minimal, especially for the non-elderly. Yet in Supplemental Table 2 of their report, Dahl et al. show that the adjusted rate of all-cause death for those that were fully vaccinated was much lower than that of the unvaccinated — the ACM was 51% lower in the 45-64 year old population (a reduction of 54% for men and 45% for women)! Similar reductions were observed when comparing the partially vaccinated group to the unvaccinated group.
The authors report reductions in ACM for all vaccinated adults compared to the unvaccinated group during this period of low COVID-19 risk, yet no commensurate reduction in all-cause mortality was observed for the overall population. Instead there was a slight increase of 3.7% during this period. Clearly the observed differences in ACM between the vaccination groups are due to inherent biases as opposed to a causal link with vaccination. Indeed, this apparent bias has been exposed in several observational studies of ACM by vaccine status.
Consider, for example, the studies cited by Dahl et al. (2024) that refute claims that vaccinations may have contributed to increased mortality risk. Closer inspection of these studies indicate that they show no such thing. What they do show is that those who received the C19 vaccine differ in fundamental ways from the group that chose not to take the injections as evidenced by large group differences in other measures that cannot plausibly be due to the vaccine.
A 2024 study by Mimura et al. (2024) out of Japan examined short-term mortality risk after mRNA vaccination after adjusting for age, sex and a set of 17 comorbid conditions; death after SARS-CoV-2 infection was excluded from the study. While the authors conclude there was no increase in (non-Covid) mortality risk following vaccination, their results actually show markedly lower adjusted odds ratios compared to the unvaccinated (especially in the ≥65-years-old population) — a reduction that cannot be attributed to the vaccines.
Xu et al. (2024) used a modified self-controlled case series (SCCS) design, adjusted for seasonality, to assess the risk of non-COVID-19 mortality, all-cause mortality, and four cardiac-related death outcomes after primary series COVID-19 vaccination in the USA over the period December 14, 2020 - August 11, 2021. Relative Incidences of non-COVID-19 mortality, all-cause mortality, and four cardiac-related death outcomes were below 1 for all three types of vaccines considered (Pfizer, Moderna and Janssen). Most of the RIs were significantly less than 1, statistically speaking.
This study is at odds with an analysis conducted by the Florida Department of Public Health in 2022 that used a SCCS design that showed males aged 18–39 years had an increased risk of cardiac-related deaths in the 28 days following the last dose of mRNA COVID-19 vaccines.
Stivanello et al. (2022) looked at the short-term mortality following COVID-19 vaccination in Bologna, Italy in the first year of vaccine rollout and compared mortality in the 3, 7, 14 and 30 days after vaccination (risk interval) with the mortality in the period of the same length (3, 7, 14 and 30 days) beyond the 30th day after the last dose of vaccination (control interval). They found that the incidence rate ratio (IRR) was significantly less than one, and that remained the case when all SARS-CoV-2 infections that occurred after vaccination were excluded and when the gender, age class, type of vaccine, period of vaccination, and a frailty index were included in the model as covariates. The authors noted that it is unlikely that the vaccine has a protective effect, especially when we excluded COVID-19 related events.
Brechje de Gier et al. (2023) examined the effect of COVID-19 vaccination on mortality by COVID-19 and on non-COVID-19 mortality in the Netherlands over the period January 2021-January 2022. They concluded that, at the population level, COVID-19 vaccination greatly reduced the risk of COVID-19 mortality and that no increased risk of death from other causes was observed. However, their analysis actually showed a much lower risk of non-COVID-19 mortality during the weeks immediately following a first, second or booster dose of vaccination as compared to that of the previous vaccination status (no vaccination, one or two doses, respectively). The authors note that “a true protective effect of COVID-19 vaccination on non-COVID-19 mortality is biologically implausible. Likely, healthy vaccinee bias has affected the results.” This, of course invalidates their conclusions regarding the impact of C19 vaccination on mortality risk.
The study by Kazem Rahmani et al. (2022) simply presents a meta-analysis of highly problematic, biased studies that have examined the incidence, hospitalization, and mortality from COVID-19 by vaccination status.
These observational studies demonstrate that the underlying assumption — that both groups have an identical baseline likelihood of dying (due to COVID or otherwise) —is erroneous. The group of individuals who received the C19 vaccine differs in fundamental ways from the group that chose not to take the injections. As such, it would be improper to conclude, or even suggest, that COVID-19 vaccination reduces the risk of COVID-19 mortality based on these study results. Likewise, the studies do not provide evidence that the vaccines carry no increased risk of death.
Many researchers point to a potential “healthy vaccine bias” as a likely reason for the reduced (non-Covid) mortality rates in the vaccinated group. Fürst et al. (2024) investigated claims of the healthy vaccinee effect (HVE) in COVID-vaccine studies and found that, consistently across datasets and age categories, ACM was substantially lower in the vaccinated than unvaccinated groups regardless of the presence or absence of a wave of COVID-19 deaths. They also found that ACMs in groups more than 4 weeks from Doses 1, 2, or 3 were consistently several times higher than in those less than 4 weeks from the respective dose. The researchers conclude that HVE is a valid concern and emphasize the importance of properly accounting for the baseline difference in the frailty of vaccinated and unvaccinated populations in periods without COVID-19 when estimating C-19 vaccine effectiveness from observational data. However, as demonstrated in some of the studies listed above, huge statistical biases may persisted (or even increase) in models attempting to control for baseline health or frailty.
Confounding & Causation
In previous writing I discussed how statistical analysis is heavily nuanced, and researchers need to be mindful of the limitations of the data they use. It is important to test the validity of underlying model assumptions and care must be taken when interpreting results. MANY studies published during the pandemic failed on these fronts. Instead, the aim of countless studies was to seek confirmation of the researchers’ biases — to seek models that fit their desired narrative instead of trying to learn from the data. And the more confounding factors there are to play with, the more leeway one has to find such a model and misinterpret the results.
When reviewing the Norwegian study, I was reminded of a study conducted by three Canadian researchers based in Toronto who investigated the link between C19 vaccine status and traffic accidents. The researchers examined government-held records of more than 11 million adults residing in Ontario and found that in the summer of 2021, unvaccinated people were 72% more likely to be involved in a severe traffic crash than those who were vaccinated (Redelmeier, Wang, and Thiruchelvam, 2023). The following excerpt is taken from the study COVID Vaccine Hesitancy and Risk of a Traffic Crash, published in the American Journal of Medicine:
“The observed risks are sufficiently large that paramedics, emergency staff, and other first responders should be aware that unvaccinated patients are overrepresented in the aftermath of a traffic crash. The observed risks might also justify changes to driver insurance policies in the future. Together, the findings suggest that unvaccinated adults need to be careful indoors with other people and outside with surrounding traffic.” — Redelmeier, et al. (2023)
Instead of recognizing that they had, in essence, conducted a falsification test and warning against making a causal link between vaccination and traffic accidents, they did the very opposite — they suggested the results justified changing insurance policies based on vaccination status!
What is driving such ill-advised counsel?
In their paper, Redelmeier et al. recite the well-known mantra: “correlation does not mean causality.” They even acknowledge the large differences in demographic and socio-economic factors between the vaccinated and unvaccinated groups and they mention many limitations of their study. BUT somehow these researchers thought it was still okay to base punitive policy on vaccination status, making the claim that COVID vaccination is an objective (!) indicator of human behavior. The many study limitations were simply presented as opportunities for further research instead of weaknesses that invalidated their conclusions.
It is prudent to note that during the time this study was completed, there was a concerted effort in Canada to paint the unvaccinated as reckless individuals who posed a disproportionate risk to others. It was a key talking point of the federal Trudeau government, mimicked in the press, and endorsed by a number of vocal researchers who received federal funds to push for greater C19 vaccine uptake. Alongside this messaging, politicians had imposed punitive measures to strip “the unvaxxed” of basic life necessities and were seeking additional ways to destroy this unwelcomed minority. And they were looking for scientific research they could use to justify such actions. Unfortunately, when it comes to pandemic science, fallacious research has been the norm in Canada.
Spurious correlations, nonsensical statistics, and fabricated results were hallmarks of “The Science” used by Canadian politicians and policy makers to justify their ineffective and harmful pandemic measures.
Rather ironically, Canada’s trove of faulty pandemic studies provides strong evidence of scientific fraud and malfeasance that has the potential to destroy the very narrative these studies sought to solidify. In a similar fashion, studies that attempt to exploit inherent differences in the vaccinated and unvaccinated populations in order to bestow phantom benefits to the COVID-19 vaccines only serve to cast further doubt on their safety and efficacy. Overt researcher bias also threatens the credibility of the researchers as well as the journals who publish the misleading conclusions.
The Bottom Line
Did the study show that C19 vaccines reduced all-cause mortality in Norway during the pandemic? NO.
The study confirmed that those who received the C19 vaccine differed in fundamental ways from the group that chose not to take the injections — something that is already well known.
Thanks for reading!
Dr. Regina Watteel is a Canadian statistician and author of the bestseller Fisman's Fraud, an exposé on the rise of Canadian hate science that was used to vilify unvaccinated Canadians and prop up COVID-19 vaccine mandates and travel restrictions.
This research is self-funded. Any support is greatly appreciated!
Good to make this critique! Good points raised.
What did the unvaccinated have in common? Prior experience to be cautious of public health and medications/medical procedures? Many indigenous populations have a history of being experimented on...