

Fudging the Numbers with the Ontario COVID-19 Science Advisory Table: Part 1
A closer look into these so-called "experts" and their unscientific ways

This post is dedicated to the many Canadians negatively impacted by COVID-19 workplace mandates. May this analysis prove useful.
“The Science Table was a self-appointed and self-important group that inserted itself into Ontario’s policy making early in the pandemic by putting forward modelling and projections on COVID. Despite being put on a pedestal by much of the media, the Science Table quickly proved themselves to be an organization that couldn’t get basic things right.” — Brian Lilley, Toronto Sun (Aug 26, 2022)
What was the Ontario Science Table (OST)?
The Ontario COVID-19 Science Advisory Table (OST) was a group of self-appointed experts with strong affiliations to the University of Toronto and numerous pharmaceutical companies that advised the Ontario provincial government on COVID-19 pandemic policy.
The Science Table was formed in July 2020 with the stated mission of evaluating and reporting on scientific evidence relevant to the COVID-19 pandemic, to inform Ontario’s response. It touted itself as a group of non-partisan, independent scientific experts that provided credible scientific advice. But, as pointed out by columnist Brian Lilley of the Toronto Sun, the Table was routinely found to get basic things wrong. Moreover, a look into its members’ affiliations reveals numerous ties to big pharma. What’s more, prominent OST members, such as former Assistant Scientific Director Nathan Stall and mathematical modeler David Fisman, routinely posted their strong partisan support and anti-Conservative views on social media. Unfortunately, the more one looks into the inner workings of the Ontario Science Table, the clearer one sees that the group was not what it purported to be. Of key concern is whether the OST provided accurate and honest information to the public and to government.
Did Ontario Science Table “experts” follow scientific methodology and provide objective, evidence-based advice to the government?
The Toronto Sun article referenced at the beginning of this post provides numerous examples of just how wildly off the Table’s COVID-19 projections turned out to be in hindsight. However, the Table’s shaky track record isn’t limited to its poor ability to anticipate future trends, but extends to their overall ability in assessing the threat of COVID-19, whether they were advising on past, present or impending events. This post demonstrates the disconnect between the facts on the ground and the narrative put forth by the OST in support of vaccine passports and mandates as the new genetic COVID-19 vaccines were rolled out to the public.
Specifically, the Table admitted that their early support for vaccine mandates and passports lacked scientific justification and that such measures raise ethical and legal concerns. However, as months passed and evidence proved the COVID-19 vaccines to be ineffective in curtailing community transmission, the Table doubled-down on their support for the discriminatory measures. A closer look into the statistics generated by the OST indicates a reliance on unscientific methodology to falsely inflate COVID-19 rates amongst the unvaccinated group relative to those of the vaccinated. The Table then used these inflated rates to encourage vaccine uptake and justify punitive restrictions against unvaccinated individuals. The gross misrepresentation of facts put forth by the Table has had serious ramifications in numerous tribunals where workplace vaccination policies have been challenged.
The Not So Scientific Ways of the Ontario Science Table
In December 2020, the new genetic COVID-19 vaccines were given interim approval in Canada and the vaccine rollout began with priority given to frontline healthcare workers, long-term care residents and the elderly. Heading into the spring of 2021, there was a large uptake in first-dose vaccinations as the new vaccines were made available to the general public. This coincided with an uptick in COVID-19 cases — a trend that had been witnessed during the vaccine rollout in many other countries as well. By May 2021, breakthrough cases had become the norm and there was growing speculation that COVID-19 vaccine mandates were on the horizon. Politicians denied such was the case, with Trudeau himself publicly assuring Canadians that “we’re not a country that makes vaccination mandatory.” A couple of months later, Ontario Premier Doug Ford ruled out implementing a provincial vaccine passport system.
“The answer is no, we're not gonna do it. We're not gonna have a split society.”
— Premier Doug Ford, July 15 2021
One week later, the Ontario Science Table undermined Ford’s position by publishing a “science brief” that urged the provincial government to act fast in creating a vaccine passport system before businesses found their own solutions that may not be as “inclusive” or “equitable.” Some academic institutions such as Seneca College, the University of Toronto and the University of Ottawa had already announced they’d be requiring their students, athletes, faculty, and staff to be vaccinated in order to return to campus in-person. The science brief, while touting the possible benefits of vaccine passports, did acknowledge that there was no actual scientific evidence to support them. Indeed, at that time there were mounting concerns about the rising number of breakthrough cases. Large outbreaks amongst mostly vaccinated venues were being reported in the media, and the CDC was warning that vaccinated people infected with the virus transmit about as much as the unvaccinated. In addition, Israel, the first country in the world to have fully vaccinated a majority of its citizens against COVID-19, was seeing a resurgence in cases and was warning other countries that two doses of the vaccines wouldn’t be enough to control transmission.
Despite these glaring red-flags, the unscientific call for vaccine passports and mandates overtook sound reasoning with those in favour of such policies displaying a growing intolerance towards anyone voicing opposition. Unfortunately, influential individuals within the medical and scientific community, including members of the OST, were amongst those leading the irrational charge. “Anti-science, anti-vaxxer” became an acceptable slur even amongst trusted professionals and, once PM Trudeau announced the federal election, it took on a life of its own. Spine-chilling calls for punitive measures against the unvaccinated escalated as Trudeau campaigned on the promise of marginalizing these so-called “anti-vaxxers.”

Upon re-election, PM Trudeau made good on his threats. He implemented vaccine mandates and travel restrictions against the unvaccinated. His government continued to encourage all employers to implement their own vaccine requirements, and the feds paid provinces to implement vaccine passports. The strong assurances made just months earlier by PM Trudeau and Premier Ford, that they would respect bodily autonomy, proved false. It is important to note that during the lead-up to the 2021 “summer of hate and division,” Canadians were prepped by aggressive back-to-back advertising campaigns encouraging them to “do their part” and get vaccinated.
The first phase of the marketing campaign, titled COVID-19 Vaccines and You, began in early March. It sought to educate and build trust in the COVID-19 vaccines. Concurrently, the federal government invested an additional $64 million in COVID-19 vaccine education campaigns to be delivered through academic institutions, hospitals and other partners in order to combat vaccine hesitancy and encourage Canadians to get the shot.
In May 2021, the second phase of the national advertising campaign began. The Ripple Effect campaign ran ads on TV and radio, in print media, on buses, digital signs, web sites, social media and through search engine marketing. The central theme was “to remind Canadians about the collective vaccination effort required to see a reduction in restrictions and public health measures.” Concurrent with the Ripple Effect campaign, the government launched the Ask the Experts campaign featuring short videos by trusted experts wherein they assured Canadians that the vaccines were “safe and effective” for everyone, even during pregnancy, and that the young and healthy also needed to get vaccinated.
A timeline of COVID-19 cases and major political events for the months following Trudeau’s election call is provided below.
Shortly after the election, by October 2021, it was generally acknowledged that any immunity imparted by the vaccines was transient and waned after a few months. Oddly enough, the Science Table took that moment in time to step forward and proclaim that there was now conclusive evidence COVID-19 vaccines were highly effective at reducing transmission. The Science Table then recommended that the Government of Ontario implement vaccine mandates for hospital workers; Premier Ford ultimately declined to do so, leaving hospitals to set their own vaccination policies. Within two months of that counsel, Omicron hit and COVID-19 cases surged to record heights. Not only did vaccinated individuals dominate the Omicron cases (as shown in the figure above), their infection rates outpaced those of the unvaccinated, as discussed in the next section.
An Inconvenient Truth
From late August 2021 to early March 2022, the Government of Ontario reported daily COVID-19 rates by vaccination status. The plot below is a screenshot from the official government website annotated with the incremental increase in COVID-19 rates amongst the vaccinated when the Omicron wave hit, as well as the relative differences in rates between vaccinated and unvaccinated before and after the surge.

As shown in the above diagram, leading up to December 2021, differences in estimated daily Ontario COVID-19 rates between the three vaccination groups were within about 10 cases in 100,000. Such differences could easily be attributed to misclassification bias, selection bias, inaccurate population size estimates and any number of confounding factors such as disparities in age, underlying health or other key attributes between the groups. Such well-known data limitations severely restrict any inferences that can be drawn regarding vaccine effectiveness. As such, it would be ill-advised to use such data as the basis for punitive, highly discriminatory public policy such as vaccine passports and mandates.
In December 2021, with about 80% of the population fully vaccinated, the Omicron variant emerged and COVID-19 rates surged in both the vaccinated and unvaccinated groups. As shown in the above diagram, infection rates amongst the vaccinated group rose well above those of the unvaccinated — a real problem for those who advocated for restrictions against the unvaccinated. That should have put an end to any restrictions based on COVID-19 vaccination status. Instead, political rhetoric against unvaccinated individuals increased and ardent pro-mandate researchers sought excuses to ignore the inconvenient real-world observations. Academic malfeasance rose to new heights in order to combat the unwelcome reality. Deceptive tactics used during this time included:
Method #1: Completely ignore real-world observations and simply fabricate the data and results wanted.
Method #2: Inappropriately manipulate the data to align with the desired trends.
Method #3: Don’t report or collect data that runs contrary to, or may jeopardize, the desired narrative.
The first method was embraced by Fisman et al. (2022) in their federally-funded CMAJ study, tailor made for the Trudeau government to “justify” extending the federal travel restrictions against unvaccinated individuals. The researchers simply concocted a mathematical model to generate data that showed the unvaccinated dominated the COVID-19 caseload and had disproportionately greater infections. They then proceeded to pass off their “findings” as fact. Mainstream media played along with the blatant fraud, blasting the faux results across the nation. I cover this in great detail in my book Fisman’s Fraud: The Rise of Canadian Hate Science. Despite strong blowback from the scientific community and a book detailing the Establishment’s involvement in the fraud, top research institutions still endorse the study and its findings. Worse, the Canadian Institutes of Health Research (CIHR) has continued to fund additional bogus pandemic studies led by Dr. Fisman, including a 2024 updated version of the fraudulent transmission study that clings to the lie that the “unvaccinated” pose a greater risk to others.
The second method — inappropriate data manipulations — is a more insidious approach, and has been the predominate technique used throughout the pandemic to misrepresent COVID-19 infections and trends in order to fit political narratives. The specific manner in which the Ontario Science Table manipulated the data to support vaccine mandates post-Omicron is covered in more detail in the sections below. When data and results are manipulated with intent to mislead or deceive it is considered falsification, an act of scientific fraud. This includes the use of biased methodology, unjustified alteration of data, misleading reporting, and cherry-picking the data to get the results wanted. The difficulty in establishing falsification is in showing intent to deceive as opposed to mere incompetence. Regarding the manipulations conducted by the OST, it is not believable that an entire table of scientific experts could consistently break with established scientific methodology unwittingly. Interestingly, Fisman was a member of the OST until stepping down in August 2021 — apparently the Table was not dialing up the COVID-19 panic enough for his liking. In addition, his co-author of the fraudulent transmission study, Dr. Ashleigh Tuite, was serving on the Modelling Consensus Table (MCT) at the time of that publication — the MCT was a partner of the OST that worked with the support of the Ontario Ministry of Health, Ontario Health, and Public Health Ontario.
The third method is to simply not collect or report inconvenient data. Prior to the emergence of Omicron, reports of COVID-19 cases and rates dominated the news. Such reports provided a constant reminder of the impending viral threat and supposed need for government intervention. As the vaccines were rolled out, these statistics were provided by vaccination status and there was a concerted effort to make the new injections appear more effective at reducing infection than they actually were. However, once Omicron hit in late 2021, these efforts were not enough to maintain that illusion, so public health authorities adjusted their reporting methods. In March 2022, Public Health Ontario (PHO) reclassified their vaccination groups, lumping the unvaccinated with the partially vaccinated population to form a “not fully vaccinated” group, while separating out individuals who were boosted from those fully vaccinated with just the primary series. This, however, only served to highlight the failure of an additional booster dose to stop infection. So, in June 2022, PHO stopped providing COVID-19 cases by vaccination group. Then, sometime between June 29th 2022 and July 15th 2022, PHO added a hand-waving disclaimer as to why, starting in December 2021 (i.e. when reported infection rates amongst the vaccinated began to outpace those unvaccinated), their case data by vaccination status should no longer be used to assess the risk of infection 😉.
The Science Table Vs Reality: Infection Rates by Age and Vax Status
The Science Table implied that comparing raw incident rates between vaccination groups was misleading since the vaccinated population is older, with disproportionately more seniors than the unvaccinated population. So, they “age-standardized” the incident rates and presented estimates of what they believed would have been observed had vaccination uptake been similar across the various age groups. They went on to use their age-standardized estimate, void of any measure of uncertainty or nuance, as the basis for their inferences and recommendations regarding vaccine effectiveness. The result of their reweighting scheme is shown below.
As shown in the short clip above, the reweighting scheme employed by the Science Table conveniently inflated the unvaccinated COVID-19 rates just enough to sit above those of the vaccinated group for the entire reporting period.
Is this “age-standardized” methodology valid? Does it actually provide a more appropriate comparison between the two groups? The answer is a resounding NO.
When doing ANY analysis, including reweighting (such as age-standardization), it is necessary to check whether the required conditions are met and to consider how the analysis will be used in order to ensure any statistical adjustments do not increase bias or lend the results to misinterpretation. Such validation is standard research practice.
Before age-standardizing the data, the following basic questions need to be considered:
Are accurate and reliable estimates of infection rates available by each age group for both the vaccinated and unvaccinated populations over the entire period under consideration? If the answer is “no”, then age-standardizing may lead to greater inaccuracy and bias.
Are the time trends and relative differences in infection rates between the vaccinated and unvaccinated populations consistent across the different age groups OR is the overall trend dominated by a particular age group? If trends are inconsistent across the age groups, then age standardizing is likely to lead to misinterpretation and misuse of the results.
Is it more appropriate to simply stratify the data by age? This is clearly the case when looking at rates of hospitalization and death since risk of severe COVID-19 changes up to a thousand-fold or more between the oldest and youngest age groups in society.
To answer these questions, I searched the Ontario COVID-19 database for case rates by vaccination status, further subdivided by age group during the Omicron surge. Unfortunately, this data is missing for the period October 3, 2021 up until March 1, 2022. However, after scouring the Wayback Machine, I found Ontario data for the period covering December 11, 2021 through to January 9, 2022 — enough to demonstrate how the Science Table’s methodology didn’t pass even the most rudimentary validity checks.
CHILDREN AGED 0-11 (December 11/21 - January 9/22):
For children 6 months to 5 years of age, the first mRNA COVID-9 vaccine wasn’t approved until July 14, 2022. As such, there are no reliable estimates of infection rates by vaccination status for this age group for the period under investigation.
For kids 5 to 11 years, COVID-19 vaccines were approved on Nov. 19, 2021, just as Omicron was emerging. By mid January 2022, about half of children aged 5 to 11 had received at least one dose of a COVID-19 vaccine. First dose vaccine uptake tapered off in late January and into early February 2022 after reaching about 55% of the population at the time. In the early days of January 2022, the first children in this age group to be considered fully vaccinated emerged. As of October 2024, the proportion of Ontario children aged 5-11 with at least one COVID-19 dose stands at just under 40% with about three-quarters of them considered fully vaccinated.
Below is a graph showing the estimated infection rates for Ontario children aged 0-11 during the Omicron surge by vaccination status. Given the significant uptake in vaccination during this period and that children testing positive for COVID-19 within 14 days of their first dose are misclassified as unvaccinated, these estimations are subject to substantial misclassification bias in favour of vaccination. Despite that advantage, infection rates amongst children who received at least one dose of the vaccine were considerably higher than those of unvaccinated children during the holiday season. This trend is consistent with the observed increases in infection rates that was witnessed throughout Canada and other countries as initial doses of the vaccine were rolled out to the general population, providing further evidence that individuals became more susceptible to COVID-19 in the days immediately following their first dose.

YOUTH AGED 12-17 (December 11/21 - January 9/22):
Below is a screenshot of Government of Ontario COVID-19 rates by vaccination status for youth aged 12-17. As shown in the diagram, infection rates amongst fully vaccinated youth were significantly higher than those of the unvaccinated during the Omicron wave.

According to provincial data, vaccinated youth had infection rates up to 70% higher than those of unvaccinated youths during the Omicron surge. Yet, many unvaccinated youth were excluded from celebrating the Christmas holidays with their peers. The Ontario vaccine passport system banned them from restaurants, theatres, gyms and other public venues. In addition, many sports teams and youth organizations had imposed COVID-19 vaccination requirements at the behest of the Canadian government and public health experts. For some youth, the decision not to take the experimental injections effectively ended their athletic aspirations. Others, such as 17 year old Sean Hartman, decided to take the “safe and effective” vaccine just so they could continue to play the sports they loved. Tragically, four days after receiving a single dose of the Pfizer vaccine (without his father’s knowledge), Sean was taken to the hospital with unusual symptoms. A month later, after playing hockey the night before, he was found dead on the floor of his bedroom.
ADULTS AGED 18-60 (December 11/21 - January 9/22):
Below are annotated screenshots from the Government of Ontario website showing COVID-19 rates by vaccination status for adults aged 18-39 and adults aged 40-59, respectively. For both age groups, rates amongst the vaccinated were substantially higher than those of the unvaccinated during the Omicron surge.
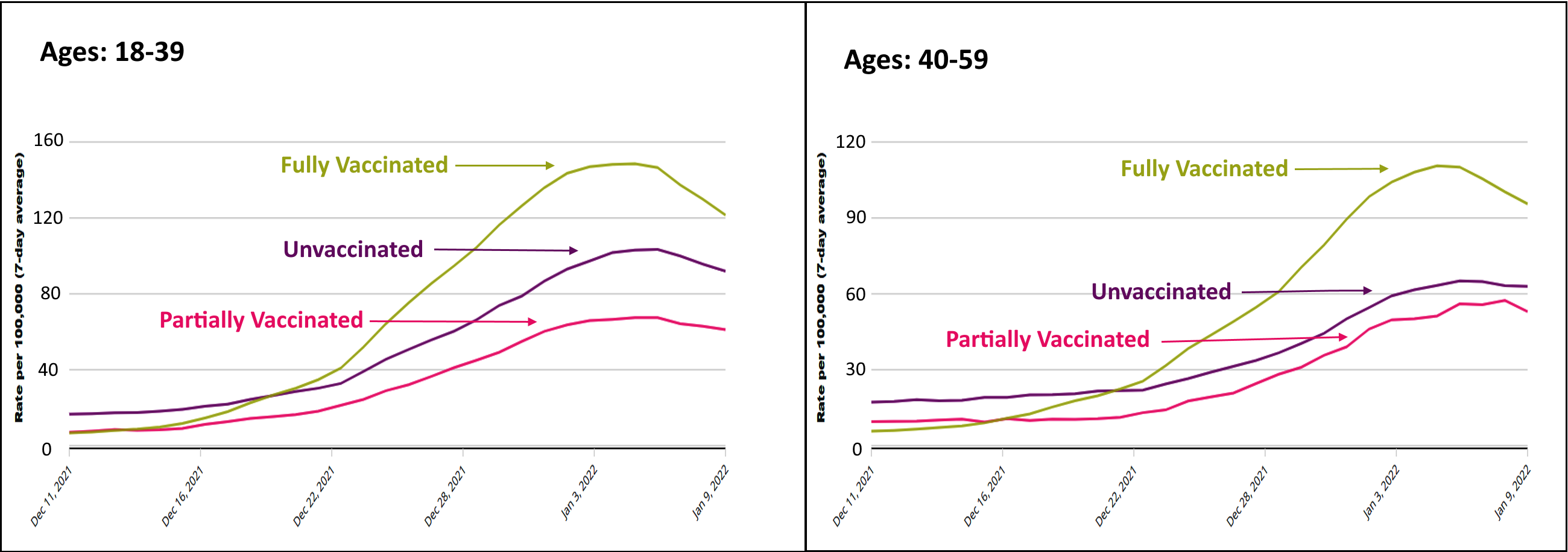
Once again, Ontario data indicates that the vaccines may have actually increased the risk of COVID-19 infection and hence transmission. That trend is consistent with data available from other parts of the world such as the UK, as well as observations from a Cleveland clinic study which found that the higher the number of COVID-19 vaccines previously received by their employees, the higher their risk of contracting COVID-19. As discussed earlier, there were MANY red flags early in the vaccine rollout that forewarned such may be the case, not to mention the fact that the vaccines were not tested on their ability to stop transmission prior to being given interim authorization by Health Canada. Nonetheless, many organizations and employers imposed vaccine requirements on their staff and/or those utilizing their services.
From the onset of the pandemic, it was understood that children and young adults were at extremely low risk of serious Covid-19. To require them to take an experimental genetic drug to participate in normal daily life is prima facie illogical and unethical. Yet, in the summer of 2021 academic institutions throughout Ontario and other provinces announced that students were required to take the novel therapeutics if they wanted to pursue a proper education, despite alarming safety signals that had surfaced. Of particular concern was the risk of myocarditis and pericarditis following vaccination, especially for young men. For the fall term 2022, months after provincial and federal governments had dropped their nonsensical vaccine passports and mandates, the Ontario Science Table continued to recommend COVID-19 vaccination for students and staff. Science Table Director Dr. Fahad Razak backed the University of Toronto’s decision to increase the number of doses required for students and employees living in residences. Dr. Razak encouraged other universities to follow suit.
By late summer, early fall of 2021 numerous workplaces had imposed vaccine mandates on their workers. At that time, the estimated infection fatality rate for people under the age of 70 was about 0.05% and, as admitted by the Science Table, there was no scientific evidence backing the discriminatory policies. By the end of 2021, real-world data indicated that, not only had authorities been wrong in their assertions that COVID-19 vaccination reduced the spread of the virus (thus affording no third-party protection to others), but that vaccination may very well be doing the exact opposite — resulting in a net public harm. The trauma inflicted by vaccine mandates should not be understated. Individuals who chose not to take the mandated injections not only endured financial hardship, but their mental health and personal relations often suffered as a result of the mandates and, for many, these stresses negatively impacted their physical wellbeing as well. And while those coerced into taking injections they didn’t want in order to keep their jobs/careers may have escaped the financial burden, many experienced a heavy psychological toll, especially if they went on to suffer vaccine injury.
Hospitals were amongst the first to implement vaccine mandates and the slowest to drop them. Many hospitals still require COVID-19 vaccination as a condition of employment. Some health care workers who were terminated due their vaccination status are still unable to find gainful employment. A recent survey of almost 500 healthcare workers in Ontario provides insight into the devastating effects COVID-19 vaccine mandates have had on the wellbeing of healthcare professionals. Many healthcare workers have left the profession due to COVID-19 policies.
Notwithstanding the above, the Science Table’s support for COVID-19 vaccination never wavered. Their reports, as well as expert testimony by former Science Table Director Peter Jüni, have been taken as fact in numerous workplace tribunals where vaccine mandates have been challenged (more on this in Part 2).
SENIORS AGED 60+ (December 11/21 - January 9/22):
In September 2022, Public Health Ontario (PHO) updated its population estimates and acknowledged that the number of unvaccinated people in the province had been greatly underestimated by roughly 400,000 — about half of which were in the senior age groups. That underestimate had a huge impact on estimated infection, hospitalization and mortality rates for unvaccinated seniors.
As shown in the charts below, in their September 11th 2022 report, PHO had estimated that 100% of seniors 70 years of age and older and 99.3% of seniors between the ages of 60 to 69 had received at least one dose of the vaccine — i.e. vanishingly few unvaccinated Ontarians over the age of 60. Two weeks later, their estimates reflected an increase of about 200K unvaccinated seniors.

The following graph shows the daily reported number of senior deaths involving COVID-19 by vaccination status provided by PHO ( 7-day moving average rates, the data can be downloaded here). The dramatic drop in deaths per 100,00 in the “not fully vaccinated” group reflects the population correction and demonstrates just how inflated and unreliable the COVID-19 statistics were for unvaccinated seniors.

Note that PHO did not go back and revise earlier COVID-19 estimates based on the corrected population sizes, nor did the Ontario Science Table, which dissolved on Sept. 6, 2022 — just weeks before PHO updated their population estimates.
The left-hand figure shown below is a screenshot from the Government of Ontario website illustrating the COVID-19 rates by vaccination status for adults aged 60-79 during the Omicron surge. The right-hand figure shows the rates when I corrected for the population size in the unvaccinated group based on PHO’s September 2022 reports.

There are several things to note from the above graphs:
Unvaccinated infection rates estimated by the government were unreliable for the senior age group.
Experts in the field of statistics and data analysis would have to have known this.
When previously underestimated population sizes are corrected based on PHO’s updated estimates, the infection rates for unvaccinated seniors are in line with those of the vaccinated.
Regarding the first two points, there are clear indicators that the unvaccinated infection rates estimated by the government were unreliable. The dramatic rise in unvaccinated rates over time as the number of vaccinated seniors in the population edges towards 100% is a clear sign of statistical instability. By early January 2022, PHO had estimated that 100% of seniors aged 70 and older had received at least one dose of the vaccine. For seniors between the ages of 60-69, the estimated vaccine coverage with at least one dose was 96.7% as of January 9th, 2022 — the last day I could find infection rates reported by vaccination status and age. No doubt PHO’s statement that they could not report this breakdown due to “technical difficulties” was a reflection of the instability of their estimates which they could no longer ignore. More importantly, “experts” on the Ontario Science Table had to have known the estimates for unvaccinated seniors were unreliable.
Just to drive that point home, PHO provided the following caveat regarding their downloadable COVID-19 vaccination data: “Coverage estimates shown as 100% may represent estimates of 100% or more. Coverage estimates may be over 100% due to limitations in the vaccination data (numerator) or Ontario population estimates (denominator).”
Indeed, when examining their data I encountered major issues with their estimates for the senior population as the number of Ontario seniors with at least one dose of the vaccine often exceeded the number of seniors in the population.
Regarding the third point, it completely destroys the Science Table’s argument that infection rates would be higher if the proportion of seniors in the unvaccinated group were similar to the proportion in the vaccinated group. The huge infection rate estimates in the 60+ unvaccinated group reported during Omicron were entirely the result of underestimating the number of unvaccinated seniors. Moreover, when population-corrected estimates are used, the infection rates amongst unvaccinated seniors were LOWER than other age-groups. So, if anything, age-standardizing the raw data and shifting more weight to the senior group would LOWER the overall infection rates during this period. That said, at the time the age-standardizing was done, the province hadn’t yet updated its population estimates. There were no reliable estimates of the infection rates amongst unvaccinated seniors available. As such, it would’ve been fallacious to age-standardize the unvaccinated data, essentially giving more weight to knowingly unreliable, highly inflated estimates.
OST Manipulations led to GREATER Misinterpretation, Bias & Misuse
As demonstrated in the above section, infection rates amongst (partially) vaccinated children, fully vaccinated youth, fully vaccinated adults aged 18-39, and fully vaccinated adults aged 40-59 were all substantially higher than their unvaccinated peers during the Omicron surge. For the senior age group there was little difference in infection rates between vaccination groups, with estimates amongst the fully vaccinated slightly above the partially vaccinated and unvaccinated populations. Rates amongst seniors 60+ were lower than other age groups.
Since vaccinated infection rates were higher than the unvaccinated across all age groups, age-standardizing the Government of Ontario data using these age classifications would preserve that overall trend and, as mentioned in the section above, serve to (slightly) lower the overall estimated infection rates in the unvaccinated. Yet, somehow, the Ontario Science Table produced rate estimates for the unvaccinated that were markedly higher than the government estimates and higher than the vaccinated rates during Omicron — that does not make numerical sense. How did the Science Table manage to pull that off? That question, along with its implications, will be examined in more detail in my next post (Part 2).
As discussed in the preceding section, in September 2022, PHO updated its population estimates and found that they had significantly underestimated the number of unvaccinated Ontarians. The figure below shows the impact of that population size correction on the Government of Ontario infection rate estimates. As you can see, the population-corrected infection estimates for the unvaccinated are notably lower than the estimates provided by the Government of Ontario, which were already substantially lower than their estimates for the vaccinated during Omicron. If this data were further corrected for misclassification bias, the unvaccinated rates would be lower still — even more so if the data were age-standardized, at least during the Omicron period.
Concluding Remarks – Part 1
The Ontario Science Table’s advice regarding COVID-19 vaccine mandates for healthcare workers, and their general support for such workplace mandates, was not evidence-based. In fact, their recommendations ran contrary to the scientific evidence available at the time. The case against these mandates has only grown stronger in the time since.
Official Government of Ontario data shows that, during the Omicron wave, the infection rates in the vaccinated population were substantially higher than those of the unvaccinated. Moreover, age-stratified data reveals that this trend was consistent for children, youth and working-aged adults, indicating that COVID-19 vaccination requirements to play sports, attend school or work was ill-advised and potentially harmful to the individual and to the greater public. That vaccination may actually increase susceptibility to COVID-19 infection was a phenomenon that had been flagged early in the vaccine rollout as a theoretical possibility.
Did real-world data justify vaccine requirements in the workplace, to attend university campus or to play sports? NO.
In stark contrast to the official Government of Ontario data, the Science Table’s COVID-19 rate estimates for the unvaccinated population are situated above those of the vaccinated for the entire reporting period. The Science Table provided no measure of the uncertainty or reliability of their reweighted estimates. Their estimates have been used as expert evidence to justify vaccine mandates and restrictions post-Omicron. The Science Table claimed that their estimates were produced by “age-standardizing” the Ontario data. However, the legitimacy of that claim is in doubt. If such methodology was used, it necessarily deviated from routine statistical practice to produce fallacious results that inflated the infection rates amongst the unvaccinated.
Was the Ontario Science Table re-weighting scheme scientifically sound? NO.
In short, the Science Table’s methodology was unscientific in nature and served to obfuscate the fact that reported incident rates amongst unvaccinated Ontarians, particularly the working aged and young, were LOWER than those of the vaccinated during the Omicron surge.
Next Up - Part 2:
Part 1 provided concrete examples of how the Ontario Science Table consistently broke with established scientific practice, distorting the facts on the ground to favour COVID-19 vaccination. Part 2 will provide additional insight into the Table’s true purpose and discuss its harmful influence on the community. Specifically, Part 2 will examine the following:
The inconsistent logic used by the OST to justify their unique take on "age-standardized" methodology that produced results contrary to standard estimation methods;
The Science Table’s terms of reference and how they acted contrary to their stated objectives;
How the Science Table influenced tribunals that challenged vaccine mandates in the workplace;
How members of the OST continue to influence advisory bodies in shaping future pandemic responses;
The real purpose behind the formation of the Science Table.
Stay tuned…
Dr. Regina Watteel is a Canadian statistician and author of the bestseller Fisman's Fraud, an exposé on the rise of Canadian hate science that was used to vilify unvaccinated Canadians and prop up COVID-19 vaccine mandates and travel restrictions.
This work is driven by a deep desire to bring about acknowledgments, accountability, protections and reparations. Any support is greatly appreciated!
Thank you for continuing to hold these groups, individuals, leaders to account. I will never ever be able to trust or forgive these people.
Lies lies lies damn bloody lies.This was a coordinated culling by governments. I know 5 people who died from these shots. Three under the age of thirty, one 55 one 60, all horrible deaths. I will never forgive nor forget, and will not be satisfied until the majority of the Politicians who were in office federally and provincially over the last four years are in prison.